A practical guide for psychologists and clinicians on writing progress notes that satisfy clinical, legal, and funding requirements without turning documentation into a second full-time job.
Progress notes are not new. Every clinician writes them. But for many psychologists, they remain one of the most time-consuming and anxiety-provoking parts of private practice.
The session ends. The next client is already waiting. There are three other notes from yesterday still unfinished. And somewhere in the back of your mind is the knowledge that whatever you write could appear in a subpoena, a Medicare audit, a NDIS plan review, or a complaint to AHPRA.
That combination of time pressure and legal exposure is why searches like psychology progress note template, how to write therapy notes fast, and what to include in a session note are so consistent. Clinicians are not looking for theory. They are looking for a structure that helps them document clearly, quickly, and defensibly — every session, every week.
This post provides exactly that.
Understanding note avoidance starts with recognising that it is rarely about laziness. Most clinicians who fall behind on documentation are not avoiding work. They are managing a specific type of cognitive pressure that accumulates across a clinical day.
Several patterns tend to drive it:
Perfectionism. The blank page asks: what is the right thing to write? For clinicians trained in careful formulation, the instinct is to get it right rather than get it done. A note that isn't perfect can sit unwritten longer than a note that simply needs to exist.
Legal anxiety. Knowing that notes can appear in complaints, audits, or proceedings creates a form of writing paralysis. The fear of writing the wrong thing sometimes produces no writing at all — which is, of course, far worse.
Decision fatigue. After five or six sessions involving high emotional load, the cognitive resources needed for clear clinical writing are genuinely depleted. This is not a character flaw. It is a physiological reality of cognitively demanding work.
Uncertainty about sufficiency. "Have I documented enough?" is a surprisingly common question, even among experienced clinicians. Without a clear internal benchmark, notes expand unpredictably or stall entirely.
Emotional residue. After a difficult session — a disclosure, a crisis, a rupture — the emotional processing required can make it hard to shift into documentation mode. The note ends up delayed not because of time, but because of what happened in the room.
Naming these patterns matters because the solution differs depending on the cause. A clinician who is perfectionistic needs permission to write a sufficient note rather than a perfect one. A clinician experiencing legal anxiety needs clarity about what defensible documentation actually requires. A clinician dealing with fatigue needs friction reduction. The later sections in this post address each of these directly.
Before focusing on format, it is worth being clear about what a progress note is for.
A progress note is not a transcript of the session. It is not a detailed narrative of everything the client said. It is a clinical record that demonstrates what happened, why clinical decisions were made, and what comes next.
This distinction matters more than it might appear. Students and anxious clinicians tend to over-document — recording everything said in the hope that more detail equals more protection. In practice, the opposite is often true. Notes that contain excessive narrative expose more information than necessary, are harder to review, and do not demonstrate clinical reasoning more clearly than a concise structured entry.
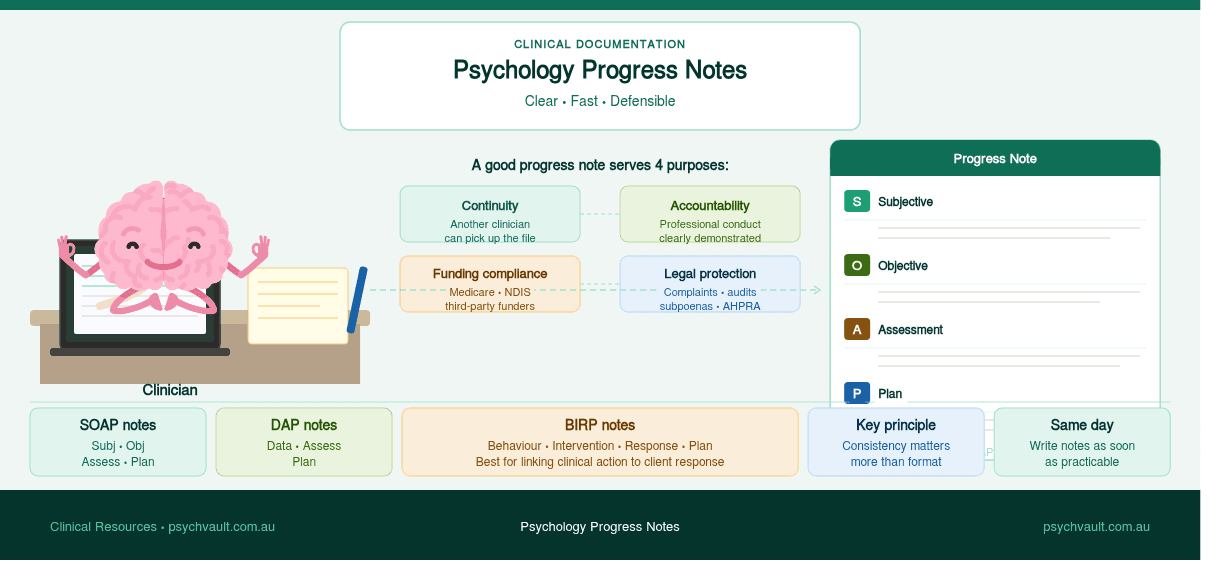
A well-written note should serve four purposes:
A note that satisfies all four purposes is not necessarily long. It is specific, structured, and clearly connected to treatment goals.
Several documentation frameworks are commonly used in psychology practice. The format you choose matters less than applying it consistently.

SOAP is the most widely recognised format across health disciplines:
SOAP works well because it separates what the client says from what you observe and interpret. This is particularly important for medico-legal purposes.
DAP is a simpler alternative that suits many psychology sessions:
DAP is faster to write and often sufficient for straightforward therapy sessions with low complexity.
BIRP is used in some mental health and community settings:
BIRP is particularly useful when you want to document the connection between your clinical action and the client's response.
Choose whichever structure fits your setting and patient population, and stick with it. Consistency matters more than format. A clinician who writes clear, consistent DAP notes will have a stronger record than one who switches formats session to session.
If you use a template, the format is largely handled for you. The real skill is in what you write inside the structure.
Regardless of format, strong progress notes tend to include the following elements.
A brief summary of how the client presented at the start of the session. This is not a verbatim account. It is your clinical observation of their mood, affect, and current situation.
Example: Client presented as fatigued and mildly dysphoric. Reported ongoing sleep disruption and a stressful workplace incident during the week. Affect consistent with reported mood. No observable distress at session commencement.
Every note should address risk, even briefly. If there are no concerns, say so explicitly. A note that is silent on risk creates an uncomfortable ambiguity if the record is ever reviewed.
Example: No suicidal ideation, self-harm, or risk to others reported or observed. Safety plan reviewed and remains in place.
What did you actually do in the session? This section should connect clearly to the treatment plan and the client's goals.
Example: Continued work on cognitive restructuring using CBT framework. Reviewed thought records completed between sessions. Identified three high-frequency automatic thoughts and examined evidence for and against each. Client demonstrated emerging ability to generate alternative appraisals with prompting.
How did the client engage with the material? Did they demonstrate understanding? Were there any difficulties?
Example: Client engaged well and noted that identifying the evidence for/against format was "more useful than she expected." Some difficulty generating alternatives in the moment; explored this as a target for practice before next session.
What is the clinical plan going forward? Include:

Notes that read like transcripts are harder to review, harder to search, and expose more information than necessary to third parties. Keep descriptions brief and clinical.
On the other end, notes like "session went well, CBT continued, client coping" are almost useless. They do not demonstrate clinical reasoning, document progress, or protect you legally.
Even a single sentence is sufficient if there are no concerns. Omitting it entirely creates a gap in the record.
Use clear language to separate what the client reported from your clinical interpretation. "Client reported feeling hopeless" is different from "client appears hopeless." Both may be true, but they are different clinical observations.
Notes should be written as soon as practicable after the session — ideally on the same day. Delayed notes can be challenged in complaints and audits, and memory fades quickly in a busy caseload.
"Client is progressing well" means almost nothing without evidence. "Client demonstrated ability to apply distress tolerance skills independently during a high-stress week, consistent with treatment goal 2" says something real.
Templates are genuinely useful — but they require active clinical thinking inside the structure. Notes that reproduce identical or near-identical wording across multiple sessions create problems in audits, complaint processes, and plan reviews.
If a funder, regulator, or legal process reviews your records and finds that twelve consecutive notes contain the same sentences with only the date changed, the natural inference is that the documentation does not reflect what actually occurred in each session. Even if that inference is wrong, it produces a record that is difficult to defend.
Templates should be starting points, not containers to fill by rote. The structure stays constant; the clinical content reflects each actual session.
One of the most useful reframes for clinical documentation is the distinction between a note that is defensible and one that is defensive.
A defensive note is written from fear. It tries to prove the clinician did nothing wrong. It over-explains, hedges, and self-protects — and in doing so, often introduces more ambiguity than it resolves. Excessive justification in a note can read as though the clinician doubted their own decisions.
A defensible note is written from clinical confidence. It documents:
A defensible note does not try to prove you are a perfect clinician. It demonstrates that you assessed appropriately, acted reasonably, documented relevant risk, and made clinically grounded decisions. That is all it needs to do.
Over-documenting out of fear creates its own risks. Notes that contain excessive emotional language, speculation about client motivation, or defensive self-commentary can be more problematic in a complaint than a clear, concise clinical record.
Write as if you are explaining your clinical reasoning to a colleague who respects your judgment. That tone — calm, specific, clinically grounded — is both more readable and more defensible than notes written under anxiety.
Most documentation advice focuses on what to write. Less attention goes to when and how — and those variables significantly affect whether notes actually get written at all.
Write on the same day. Notes written within an hour of a session are more accurate, faster to produce, and more legally sound than notes reconstructed two days later. Same-day notes take less cognitive effort because the session is still live in working memory.
Start with dot points, refine later. Jotting five rough bullet points immediately after a session takes sixty seconds. Expanding them into a full note at the end of the day is much easier than starting from scratch. The blank page is the hardest part.
Batch similar tasks. Some clinicians write notes immediately after each session. Others block twenty minutes at the end of the day. Neither approach is wrong — but inconsistency is. Find a rhythm and protect it in your schedule.
Use a template and stay in it. A template removes the format decision from every session. The cognitive effort goes into clinical content, not structure. Evaluate your template annually to make sure it still fits your setting and client population.
Try voice-to-text for first drafts. Dictating a note immediately after a session while walking to the next room takes two minutes. Most voice-to-text tools produce workable first drafts that need only light editing. For high-volume practices, this is worth trialling.
Set a sufficiency bar, not a perfection bar. A note is finished when it answers: what happened, what I did, how the client responded, and what comes next. If it answers those four things clearly, it is done.
If you are billing Medicare under a Mental Health Treatment Plan, your notes are part of the evidence trail that justifies the rebate. They should clearly show that you provided a psychological therapy session with appropriate clinical content, not just a supportive conversation.
For NDIS participants, progress notes often feed into plan reviews, reports to support coordinators, and evidence for ongoing therapeutic support funding. Notes that track functional progress over time — not just session content — are significantly more useful in those contexts.
If a funder or regulator can read your notes and understand what changed for the client and why your work contributed to that, the notes are doing their job.
If NDIS documentation is part of your workload, pair this article with the NDIS report template checklist and the reasonable and necessary NDIS criteria guide. Progress notes are often the raw material those later reports rely on.
For private health fund billing, consult your insurer's requirements. Some require specific wording or minimum content standards for session notes.
Telehealth sessions should be documented in the same way as in-person sessions, with two additions:
This matters for Medicare compliance and medico-legal purposes. Some clinicians also note any technology difficulties that affected session delivery.
A well-designed template is not a shortcut that reduces clinical thinking. It is a structure that ensures you capture the right information without having to reconstruct the format from memory after every session.
The best templates prompt you through each required section, leave enough space for real clinical content, and are formatted so the note reads logically whether it is reviewed on screen or printed.
PsychVault has a range of clinical documentation templates built specifically for Australian psychologists and allied health practitioners — including progress note templates formatted for different practice settings and client populations. If you do not see what you need there, or you can build something better for your niche, become a creator on PsychVault and earn from resources that help other clinicians work more clearly.
When evaluating any template, check that it covers:

Before saving or submitting a progress note, run through this quick check:
If yes to all seven, the note is doing its job.
How long should a psychology progress note be?
A progress note should be long enough to document what matters and short enough to complete within a reasonable time. Most well-structured notes are 150–400 words. Aim for notes you can write in 5–10 minutes; notes that take much longer usually indicate a structural or clarity problem with the template or workflow.
What is the minimum requirement for psychology progress notes under AHPRA?
AHPRA requires adequate records of each client contact. The record must be sufficient for another practitioner to understand the client's history, current presentation, and treatment status. There is no mandated word count, but inadequate records are a common finding in professional conduct proceedings and health complaints investigations.
Can I use a template for psychology progress notes?
Yes. Progress note templates are widely used in Australian clinical practice and are encouraged as a way to ensure documentation consistency. A good template prompts you through required sections while leaving room for specific clinical content. The goal is a structured note, not a generic one.
How soon after a session should I write a progress note?
AHPRA guidelines and good clinical practice strongly recommend writing progress notes on the same day as the session, ideally immediately after. Delayed notes are less accurate, carry greater medico-legal risk, and may be challenged in professional conduct or insurance contexts.
What should a telehealth progress note include beyond a standard note?
Telehealth notes should include all standard progress note elements plus: the platform used (e.g., Coviu, Zoom), confirmation that the client consented to telehealth delivery for that session, and any technology issues that materially affected session delivery. This is required for Medicare telehealth item compliance.
Progress notes are not paperwork to get through as fast as possible. They are part of professional practice, legal protection, and continuity of care.
The goal is not to write long notes. It is to write notes that are clear, specific, and clinically grounded — notes that demonstrate your thinking without becoming a burden on the rest of your day.
A reliable structure, a clear sufficiency benchmark, and a consistent habit of writing same-day notes will take most of the cognitive drag out of documentation.
The best progress notes are not the longest ones. They are the ones that still make clinical sense six months later when someone else has to read them — clear enough to follow your reasoning, specific enough to show what actually changed for the client, and grounded enough to stand on their own if they ever have to.
For broader template selection, see Practical psychology templates for therapy, assessment, and NDIS work. If you are building client-facing resources rather than practitioner notes, the psychoeducation handouts guide covers a different but related design problem.
Share your thoughts and experiences with this resource.
Sign in to leave a comment
Move from strategy into implementation with templates, handouts, and psychoeducation tools already live on the marketplace.
Publish clinician-grade templates, build trust signals, and start growing an evergreen library under your own brand.
A practical guide to the psychology templates clinicians use most — CBT worksheets, intake forms, case formulation, behaviour support, and NDIS documentation.
A practical guide for Australian psychologists and allied health clinicians on what neuroaffirming documentation actually means, and how to spot it in the resources you use.
A practical checklist for writing clearer NDIS psychology reports — stronger functional wording, cleaner recommendations, and less admin for Australian clinicians.