A practical and honest guide for neurodivergent psychologists and allied health clinicians navigating systemic ableism, masking, burnout, and finding environments where they actually thrive.
There's a particular kind of exhaustion that comes from being a neurodivergent clinician in a neurotypical profession.
It's not the exhaustion of the work itself - the clinical hours, the case formulation, the supervision. It's the exhaustion that sits underneath all of that. The constant translation. The performance of competence in forms that don't fit your brain. The smile you hold through a microaggression about your handwriting. The three hours you spent rewriting a report that would have taken a neurotypical colleague forty minutes.
The psychology profession is extraordinarily good at talking about neurodivergent clients. It is considerably less good at talking about neurodivergent clinicians. This guide is for us.
Jump to a section:
Psychology as a discipline has made significant progress in understanding neurodivergence. Autism, ADHD, dyslexia, dyspraxia, PDA - these are increasingly understood through a neurodiversity lens rather than a purely deficit-based medical model. Identity-first language is becoming standard. Neuro-affirming practice frameworks are emerging.
And yet.
The profession that produces these frameworks, that trains clinicians in neuro-affirming approaches, that advocates loudly for its neurodivergent clients - often fails its neurodivergent clinicians in quiet, persistent, and sometimes devastating ways.
The expectation that everyone can write quickly by hand. The back-to-back caseloads that assume consistent cognitive output across eight hours. The open-plan offices. The unwritten rule that supervision should feel natural and conversational. The assumption that administrative burden is equally distributed across all neurotypes.
These aren't edge cases. They're structural features of how clinical workplaces are typically organised - and they reflect an unexamined assumption that the neurotypical clinician is the default.
This guide names that assumption, examines its consequences, and offers practical strategies for neurodivergent clinicians navigating a profession that wasn't designed with them in mind.
It also matters to say early that this is not only a problem story. Environment fit and population fit are professional sustainability issues, not indulgent preferences. Many neurodivergent clinicians do some of their best work precisely in the areas where lived experience, direct communication, systems thinking, or recognition of masking become clinical assets rather than liabilities.
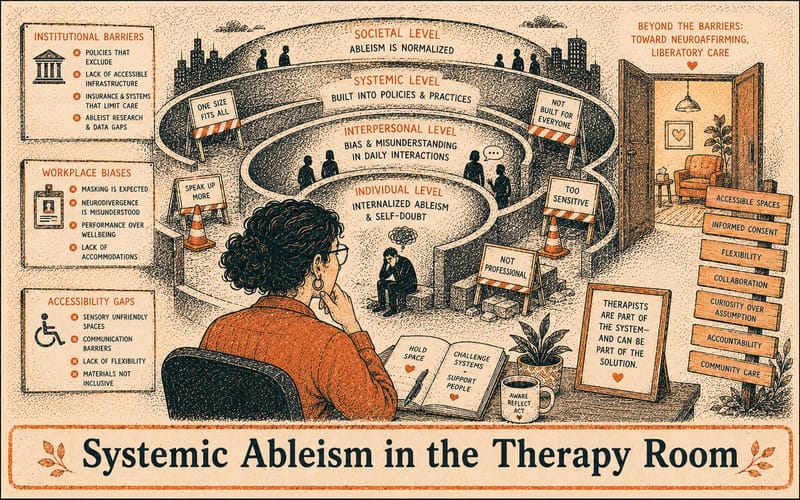
Systemic ableism isn't usually dramatic. It doesn't announce itself. It shows up in the texture of everyday clinical work - in policies, expectations, and physical environments that were designed without neurodivergent clinicians in mind.
One of the most persistent and least examined examples: the expectation that clinicians take handwritten notes during sessions.
For a clinician with dysgraphia, handwriting under time pressure is genuinely difficult - and requiring it in a clinical context isn't just inconvenient, it actively degrades both the clinician's experience and the quality of their documentation. A clinician who is struggling to form legible letters is not simultaneously attending to their client with full capacity.
Alternatives exist. Voice-to-text. Typed notes immediately post-session. Digital stylus. Audio recording with consent. Most of these alternatives produce better documentation outcomes for everyone. But many workplaces default to handwritten notes because that's how it has always been done - and changing the default requires someone to name the problem first.
The dysgraphia example is specific, but it illustrates a broader pattern: clinical workplaces frequently have arbitrary requirements that reflect neurotypical norms rather than genuine clinical necessity. The question worth asking of any administrative requirement is: does this requirement serve the client's care, or does it serve convention?
The standard private practice model - eight clients a day, back to back, with fifteen-minute gaps for notes - is cognitively demanding for any clinician. For neurodivergent clinicians, particularly those with ADHD or autism, it can be genuinely unsustainable.
Sustained attention across multiple client presentations requires significant executive function. Context-switching between presentations requires cognitive flexibility that is unevenly distributed across neurotypes. The fifteen-minute gap that is theoretically for notes becomes, in practice, a sensory and cognitive recovery period - which means the notes don't get written, the backlog builds, and the clinician ends the day exhausted and behind.
This isn't a motivation problem. It's a mismatch between caseload architecture and cognitive architecture.
Sensory environments matter. For autistic clinicians and those with sensory processing differences, open-plan offices - the standard configuration in many community mental health and allied health settings - can be genuinely aversive. Fluorescent lighting, background noise, unpredictable interruptions, and the cognitive load of monitoring social dynamics in a shared space all extract a toll that neurotypical colleagues may not notice or understand.
This toll doesn't disappear at the end of the workday. It accumulates.
Clinical workplaces have an unspoken model of what a competent clinician looks like. They're verbally fluent in supervision. They produce notes quickly and legibly. They manage their caseload without visible difficulty. They respond to emails promptly. They present as organised and on top of things.
This model is neurotypical. And it functions as an invisible standard against which neurodivergent clinicians are constantly measured - often by supervisors who don't recognise they're doing it.
Microaggressions toward neurodivergent clinicians are rarely malicious. They're usually well-intentioned comments that land badly because they reveal an underlying assumption - that neurodivergence is a personal failing rather than a neurological difference.
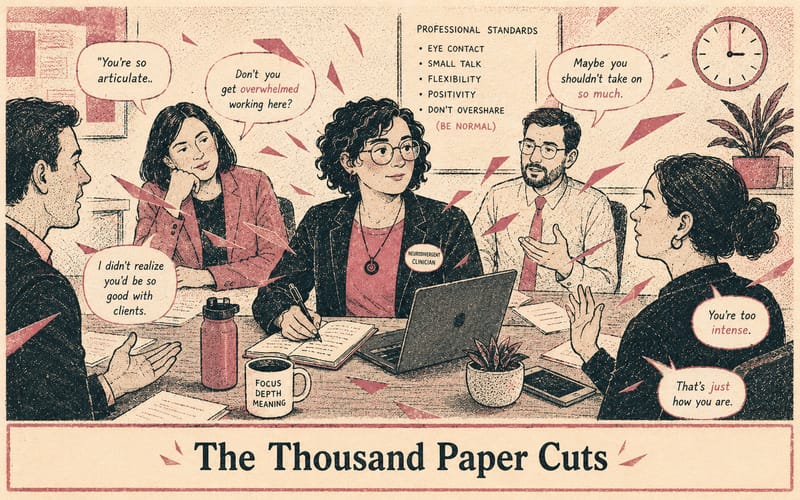
Some of the most common:
"You don't seem dyslexic."This one is a double-edged dismissal. It simultaneously invalidates the diagnosis and implies that dyslexia has a visible presentation - that it should be detectable from the outside. What it actually communicates: your experience of disability is only valid if it matches my expectations of what disability looks like.
"Everyone finds supervision overwhelming."Said in response to a disclosure that supervision feels particularly demanding. The intention is usually reassurance. The effect is erasure - the specific difficulty of a neurodivergent clinician navigating supervision is flattened into a universal experience that doesn't require accommodation.
"You just need to get more organised."Said to a clinician with ADHD whose documentation is behind. As if organisation is a choice rather than an executive function challenge. As if the solution to a neurological difference is trying harder.
"Are you sure you're cut out for this?"This one is less common but more damaging. Usually said in a moment of frustration, often by a supervisor who has conflated professional struggle with professional unsuitability. For a late-diagnosed neurodivergent clinician who has spent years doubting themselves, this question lands in a very particular way.
"You were fine last week."Said when a clinician's output varies - good days and bad days, high-energy periods and crashes. This comment reflects a misunderstanding of how variable neurodivergent performance can be, and implies that inconsistency is suspicious rather than neurological.
"But you're slow at documentation."Said without context, as if documentation speed is a neutral baseline rather than a variable shaped by working memory, dyslexia, dysgraphia, perfectionism, or the need to think through structure explicitly rather than intuitively. What it communicates: output speed matters more than judgement. What it often misses: many neurodivergent clinicians produce thoughtful, detailed documentation precisely because they cannot shortcut the process in the way others can.
These comments accumulate. Each one is small. Together, they communicate a consistent message: you are not quite right for this profession. That message is false, and it is harmful.
Masking - the conscious or unconscious suppression of neurodivergent traits to appear neurotypical - is well documented in autistic and ADHD research. It is less discussed in the context of clinical workplaces, where the stakes of being perceived as incompetent are professional rather than just social.
Neurodivergent clinicians mask in specific ways:
Performing confidence in supervision. When you're unsure, when you're struggling, when the case is genuinely difficult - but you present as collected because you've learned that uncertainty is read as incompetence.
Over-preparing to compensate. Spending four times as long on a report as a neurotypical colleague because you know your first draft won't be adequate. Working evenings to catch up on documentation that fell behind during the day. Arriving early to read through files before sessions because your working memory doesn't retain detail the way others seem to.
Suppressing self-regulation behaviours. Stimming, movement, fidgeting - all the things that actually help regulate your nervous system - because clinical environments have an implicit expectation of stillness and composure.
Fawning with supervisors. Agreeing with clinical formulations you're not sure about. Not raising concerns about workplace practices that aren't working for you. Performing gratitude and compliance because you've learned that visibility as a struggling clinician has consequences.
The cost of sustained masking is significant and well-evidenced: burnout, anxiety, depression, and a gradual erosion of the self-knowledge that makes someone a good clinician. You cannot be attuned to your clients when you're spending your cognitive resources performing neurotypicality.
Late-diagnosed neurodivergent clinicians carry an additional burden: years of masking before they even had a framework for what they were doing. The diagnosis doesn't undo the exhaustion. It just explains it.
One of the most overlooked drivers of burnout in neurodivergent clinicians is that many workplace expectations are built around neurotypical functioning assumptions - and those assumptions are rarely neutral.
They often assume consistent daily executive function, linear productivity, low cognitive load in routine decisions, minimal sensory or social friction, and effortless task-switching across contexts. For many neurodivergent clinicians, none of these are stable realities.
This is why burnout is so often misread. From the outside, it can look like poor organisation, low resilience, or not coping with a normal workload. In practice, it is often cumulative executive function depletion from trying to meet a professional standard that was never designed for your brain in the first place.
What looks like a small task externally can carry significant hidden load internally. Choosing clothing for work, for example, may not be a neutral five-minute decision. It can involve sensory calculation, social calibration, memory, and impression management all at once: is this comfortable enough for a full day, is it professional enough, did I wear something too similar last time, will I stand out, am I underthinking this, or overthinking it? Those micro-decisions cost energy before the workday has even started.
The same is true for replying to emails, prioritising tasks, switching between clinical and administrative roles, and monitoring how you are being perceived in meetings, supervision, or shared office space. None of these are really "little things" if your brain is already doing more background processing than the environment recognises.
This matters because life cannot be all school or all work. A nervous system that is constantly adapting and compensating needs genuine recovery and genuine variation, not just more efficient productivity.
Sleep, food, hydration, rest, and movement matter. They matter for everyone, and they matter especially when your brain is already working harder than most people can see. Regular exercise, adequate sleep, eating properly, drinking enough water, and basic physiological regulation all support emotional regulation, cognitive capacity, and the biological conditions associated with neuroplasticity, including brain-derived neurotrophic factor (BDNF).
But this is where generic burnout advice becomes too simplistic.
Take an ADHD clinician arriving at work. Before the first session, some of their cognitive budget may already have been spent on sensory and social decisions about clothing, commuting while managing attention, walking into open-plan noise, seeing a visible email backlog, and carrying anticipatory anxiety about supervision or unfinished notes. A colleague may arrive at that same first session having spent far less of their available cognitive capacity on the pre-work layer. Sleep and exercise matter, but they do not close that kind of daily gap on their own.
Neurodivergent burnout is not just a failure to look after yourself well enough. Self-regulation supports capacity, but it does not remove structural load. You can do all the "right" things and still burn out if your days are built around relentless task-switching, sensory friction, and performance against neurotypical expectations.
That does not make the basics unimportant. It makes them foundational rather than curative.
Boundaries are often described as relational tools. For neurodivergent clinicians, they are also cognitive load management systems.
Clear boundaries reduce decision fatigue, prevent unnecessary role-switching, limit emotional and sensory overload, and protect recovery time between demands. They keep you safe not just relationally, but neurologically.
This can mean protecting transition time between clients, refusing caseload structures that leave no decompression space, limiting the number of professional roles you are juggling at once, or recognising that saying yes to everything is often a fast route to collapse rather than a sign of dedication.
Another underestimated protection against burnout is diversified engagement.
A life organised entirely around work or study increases burnout risk because it removes novelty, attention reset, identity flexibility, and emotional replenishment. Many neurodivergent people function better, not worse, when they have more than one area of interest at once.
Sustainable functioning often depends on having more than one domain of meaning. Work matters. Study may matter. But so do hobbies, movement, rest, relationships, creative interests, and whatever else reminds your nervous system that life is not one long performance review.
Many neurodivergent clinicians gravitate toward specific client populations - and this isn't accidental.
There is a particular clinical resonance that comes from shared experience. An autistic clinician working with autistic clients brings something that no amount of training can fully replicate: an embodied understanding of what it feels like to process the world differently, to be misread constantly, to have your experience invalidated by people who mean well.
This isn't to say that neurotypical clinicians can't work effectively with neurodivergent clients - they can, and many do. But the fit between a neurodivergent clinician and a neurodivergent client is worth naming explicitly, because it is a genuine clinical asset that workplaces often fail to recognise or leverage.
Populations where neurodivergent clinicians frequently report strong clinical fit:
Autistic and ADHD clients. The obvious match. But worth being specific about why: not just because of shared experience, but because neurodivergent clinicians are often less likely to pathologise difference, more likely to use direct communication, and better equipped to recognise masking in clients because they recognise it in themselves.
Late-diagnosed adults. The experience of receiving a diagnosis as an adult - the grief, the recontextualisation of your entire history, the complicated relief - is something a late-diagnosed clinician understands from the inside.
Trauma presentations. Many neurodivergent people have trauma histories connected to their neurodivergence - school experiences, workplace failures, relationships that ended because of misunderstood differences. A neurodivergent clinician who has done their own work can hold this with particular skill.
LGBTIQA+ clients. There is significant overlap between neurodivergent and LGBTIQA+ populations, and neurodivergent clinicians often share an understanding of what it means to exist outside dominant social frameworks - to have an identity that requires explanation, accommodation, and advocacy.
Clients who have been failed by systems. Neurodivergent clinicians who have navigated difficult institutional experiences often bring a systems-aware perspective that resonates with clients who feel failed by mental health, education, or workplace systems.
This fit matters for placement decisions, for caseload design, and for how neurodivergent clinicians advocate for themselves in clinical workplaces. Knowing your population strengths is not self-indulgent - it's clinical intelligence.
Not all clinical environments are created equal. For neurodivergent clinicians, environment fit is not a preference - it's a professional sustainability issue.
This is the most important and most underestimated factor. A workplace that espouses neuro-affirming values for clients but treats its neurodivergent staff as problems to be managed is not a safe environment. Values alignment means the organisation's approach to neurodivergence is consistent - it applies to clients and clinicians alike.
Signs of genuine values alignment:
Signs of values misalignment:
Private practice offers the most structural flexibility - you control your caseload size, your hours, your physical environment, and your administrative systems. For many neurodivergent clinicians, private practice, even part-time, is the most sustainable long-term model because it removes the neurotypical workplace as a constant variable. The trade-off is isolation, income variability, and the administrative burden of running a small business.
Community mental health typically offers more peer support, structured supervision, and population diversity - but comes with higher caseloads, less environmental control, and institutional processes that may not flex easily for neurodivergent staff.
Hospital and inpatient settings are high-sensory, fast-paced environments that suit some neurodivergent clinicians, particularly those who thrive with structure and clear protocols, and genuinely don't suit others. The unpredictability of inpatient work can be both stimulating and dysregulating depending on your profile.
Telehealth deserves specific mention. For many neurodivergent clinicians, telehealth removes significant sensory and social overhead - no commute, controlled physical environment, less ambient noise, ability to have your own tools and systems immediately accessible. It also removes some of the performance load around professional appearance that in-person workplaces can require. Many neurodivergent clinicians report that telehealth significantly reduces their daily exhaustion.
Part-time caseloads are not a compromise - for many neurodivergent clinicians, they are the configuration that allows genuinely excellent clinical work. A clinician seeing fifteen clients a week with full cognitive presence is providing better care than a clinician seeing thirty clients a week in a state of chronic depletion.
This is worth saying explicitly because many neurodivergent clinicians carry shame about needing a smaller caseload. The shame is misplaced. Sustainable practice is good practice.
Caseload structure matters as much as size. Spacing sessions, building in protected admin time, and clustering similar presentations can all reduce cognitive switching costs significantly.
If you're autistic or have sensory processing differences, your physical workspace is a clinical tool. A workspace that dysregulates you is a workspace that degrades your clinical capacity.
Practical considerations:
These aren't luxuries. They're the conditions under which good clinical work is possible.
These are not theoretical accommodations. These are tools and approaches that neurodivergent clinicians actually use.
For clinicians with dyslexia or dysgraphia, documentation systems matter more than generic advice about "being organised." Practice management software with robust templating - like Zanda - can be genuinely transformative. A strong template means you're not generating structure and content at the same time. The framework already exists, so more of your working memory stays available for the clinical substance.
Voice-to-text can do the same thing, but only when the surrounding workflow makes it usable. An autistic clinician with working memory differences may benefit from dictating notes immediately after a session while the content is fresh - but only if the workplace has a secure process for recording, transcribing, storing, and integrating that material into practice software. Without that infrastructure, voice-to-text can become one more workaround rather than a real adaptation.
For a practical structure, see How to write psychology progress notes. If the issue is broader resource design, the neuroaffirming templates guide explains why standard clinical templates often create unnecessary cognitive load.
Assistive technology belongs here too: text-to-speech for dense reading, grammar tools for written work, digital stylus instead of handwriting, and reminder systems detailed enough to support sequential tasks. None of this is cheating. It is infrastructure. The adaptation is not the app by itself. It is the system that makes the tool usable within actual clinical work.
Many neurodivergent clinicians who describe burnout are describing a workload architecture problem rather than a professional fit problem. If you are chronically exhausted and your caseload is full-time, trying part-time before trying to leave the profession is often a clinically sensible experiment.
The same applies to boundaries that reduce hidden load:
These boundaries are not laziness. They are intelligent conservation of cognitive resources.
The basics matter here too. Sleep, food, water, rest, and movement are often the first things to collapse when a neurodivergent clinician is overextended. If you are tired enough, everything gets harder: emotional regulation, sensory tolerance, decision-making, documentation, supervision, and task-switching. Exercise is not a cure for structural ableism, but it can support mood regulation, stress tolerance, and the brain processes associated with BDNF and recovery.
A life bigger than work matters for the same reason. Hyperfocus and vocational intensity can make all-work or all-study living feel normal for a while. It usually is not sustainable. Protecting other areas of interest is often what keeps clinical work possible over the long term.
Supervision can be cognitively demanding for neurodivergent clinicians, particularly those with working memory difficulties or PDA profiles where unstructured demand can feel aversive. A structured supervision agenda - prepared in advance and shared with your supervisor - changes the task from improvised performance to organised discussion.
If you are still choosing or evaluating a supervisor, What Good Supervision Actually Feels Like and How to find a board-approved supervisor for your 5+1 internship are useful companion pieces.
Batching admin can have the same effect. Doing one note, then seeing a client, then checking emails, then returning to another note is usually more expensive than batching similar tasks together. Notes at end of day, logbook entries on Friday afternoon, and emails at a set time can reduce the number of cognitive mode-shifts required.
Disclosure is also a systems issue, not just a personal courage issue. There is no universal right answer. Before disclosing, ask: Does this workplace support neurodivergent staff well? Does my supervisor understand neurodivergence as difference rather than deficit? What specific adjustments do I need, and are they realistic to request here? Disclosure does not have to be all-or-nothing. It can be selective, specific, and tied to practical needs rather than identity performance.
This section is for supervisors, clinical directors, and anyone responsible for the professional environment neurodivergent clinicians are working in.
Make reasonable adjustment processes genuinely accessible. If accessing an adjustment requires a formal application, HR involvement, and a waiting period, most neurodivergent clinicians will not access it. Build flexibility into the default rather than making accommodation the exception.
Review your documentation requirements critically. Ask of every administrative requirement: does this serve clinical quality, or does it serve convention? Handwritten notes, specific report formats, real-time documentation - examine each one for whether it is genuinely necessary or simply habitual.
Train supervisors in neuro-affirming supervision. Supervision models were largely developed without neurodivergent clinicians in mind. A supervisor who understands how to adapt supervision for different cognitive profiles - who can flex between structured and exploratory approaches, who doesn't read preparation as rigidity or variable performance as unreliability - is a clinical asset.
Stop conflating presentation with competence. A clinician who is quiet in team meetings, whose notes take longer to produce, who needs more structured supervision - these are not signs of clinical unsuitability. They are signs of a neurotype that requires different conditions to do excellent work.
Create physical environments that work for more brains. Quiet spaces, flexible lighting, private decompression areas, sensory considerations in workspace design. These benefit all staff, not just neurodivergent ones.
Question neurotypical baselines rather than treating them as neutral. If your workplace assumes the right clinician is the one who can tolerate endless context-switching, maintain identical output every day, make hundreds of micro-decisions without fatigue, and present effortless professionalism at all times, you are not measuring competence. You are rewarding fit with an unexamined neurotype.
Model disclosure safety. If leadership never discloses, if neurodivergent staff who do disclose experience negative consequences, if the workplace culture treats difference as a weakness - neurodivergent clinicians will mask indefinitely and burn out quietly. Safety for disclosure has to be demonstrated, not just stated.
The most important reframe in all of this is that neurodivergent clinician burnout is not usually a sign that the clinician is unsuited to the profession. More often, it is a sign that the workload architecture, supervision structure, documentation expectations, or sensory environment are mismatched to how that clinician's brain works.
That matters because it shifts the question. The question is not simply "how do neurodivergent clinicians cope better?" It is "what kinds of clinical systems produce sustainable work for different kinds of brains?"
Some neurodivergent clinicians will need smaller caseloads. Some will need different documentation tools. Some will need more structured supervision, more recovery time, more flexible environments, or more than one area of meaning outside work to stay well. None of that is evidence of lesser professionalism. It is evidence that professionalism was never a neutral standard to begin with.
The profession does not get better by asking neurodivergent clinicians to approximate neurotypical functioning more convincingly. It gets better by designing workplaces, supervision, and expectations that recognise variation as real. That is the level at which meaningful change happens.
Identity-first language is used throughout this article intentionally. Written by Ethan Smith - provisional psychologist, neurodivergent clinician, and founder of PsychVault.
Share your thoughts and experiences with this resource.
Sign in to leave a comment
Move from strategy into implementation with templates, handouts, and psychoeducation tools already live on the marketplace.
Publish clinician-grade templates, build trust signals, and start growing an evergreen library under your own brand.
A clinical guide to autistic burnout, PDA-profile demand avoidance, masking, shutdown, skill loss, recovery time, and why demand reduction is often treatment.
A clinician-facing account of PDA-style resistance through predictive processing, salience network gating, precision weighting, autonomy, and clinical formulation.
A comprehensive, evidence-informed guide to why hormonal fluctuations can magnify ADHD, autism, PTSD, anxiety, depression, OCD, BPD, eating disorders, sensory overload, and cyclical capacity loss.